23
____________________________________________________________
DIABETES AND HYPOGLYCEMIA
Diabetes and its opposite counterpart, hypoglycemia, are diseases caused by disturbances in the delicate balance of the sugar chemistry of the body. The sugar, glucose, is a normal blood constituent and is used by the body as a source of energy. To utilize this energy the body requires insulin and some 20 enzymatic chemical reactions.
For the normal functioning of the human body, the concentration of glucose in the blood must be maintained within narrow limits (the normal range is 80 to 120 mg %). The biochemical traffic policeman that controls the level of glucose in the blood is insulin. Insulin is produced in a part of the pancreas called the Islets of Langerhands, from where it enters the bloodstream.
Since the amount of glucose in the blood may vary, such as after eating, the insulin must be doled out by the pancreas in just the right amounts. Too little insulin circulating in the blood permits the glucose levels to rise (hyperglycemia) and brings on the diabetic state. When the blood level of glucose rises above the height of the kidney dam of 170 mg % (kidney threshold) it spills over into the urine and positive urinary sugar tests result. Too much insulin in the blood is equally bad because it produces the condition of hypoglycemia (low blood sugar) and there are probably as many people suffering from this serious condition as from diabetes.
In the treatment of diabetes, insulin is injected because, if given orally, it is destroyed by the digestive enzymes. The dosage of insulin requires careful control because if it is too much, low bloodsugar, or "insulin shock," will result. A test used to determine whether pancreatic secretion of insulin is normal or not is the so-called glucose-tolerance test. A large amount of glucose sugar is fed the fasting patient. The blood glucose values are determined before and at hourly intervals after ingesting the sugar. From the result obtained it is possible to distinguish normality, diabetes (too little insulin), and hypoglycemia (too much insulin). If the body has an excess of sugar beyond its immediate needs, it is converted to the insoluble carbohydrate, glycogen, which is deposited in the liver for storage. Thus a sugar reserve is available and, in times of need, glycogen can be converted back into the soluble sugar, glucose.
An estimated 4 million Americans have diabetes and about 1/2 of these are undiagnosed. Heredity is important because, in about 50 percent of the cases, there is a familial history of diabetes. It has also been estimated that about 22 percent of the United States population carries the recessive gene for this disease. Diabetes ranks eighth as a cause of death in the United States and it is the third leading cause of blindness. The importance of maintaining the delicate biochemical balance of insulin, therefore, cannot be underrated. The use of insulin for the treatment of diabetes began in the 1920s and the Canadians, Frederick Banting and John Macleod, received the 1923 Nobel Prize in Biochemistry for its discovery.
Not long after the discovery of ascorbic acid in the early 1930s, tests on guinea pigs indicated that ascorbic acid had a profound influence on the body's sugar utilization. In 1934, C.G. King and coworkers (1), at the University of Pittsburgh, showed that guinea pigs maintained on low levels of ascorbic acid developed degeneration of the Islets of Langerhands. Guinea pigs depleted of ascorbic acid showed a low glucose tolerance which was rapidly regained on feeding them ascorbic acid. In 1935 and 1937, they also demonstrated that injection of sublethal doses of diphtheria toxin (increased stress) further diminished their tolerance to sugar in proportion to the length of their ascorbic acid deprivation.
These results were confirmed and extended in a comprehensive series of papers from India by Banerjee (2), starting in 1943. He not only confirmed that guinea pigs with scurvy showed poor sugar tolerance, but indicated that the insulin content of the pancreas of scorbutic guinea pigs is reduced to about 1/8 that of normal guinea pigs. He observed gross changes in the microscopic appearance of sections of the pancreas from scorbutic guinea pigs. The appearance returned to normal when the guinea pigs were given ascorbic acid. He also reported that the normal conversion of excess sugar into glycogen reserves for liver storage is also impaired in scurvy. In 1947, using improved laboratory techniques, he confirmed his earlier results and revised his estimate of the insulin content of the pancreas of scorbutic guinea pigs to one-quarter that of normal. He also states in this paper:
The disturbed carbohydrate metabolism as seen in scurvy is due to a deficiency of insulin secretion and a chronic deficiency of this vitamin may be one of the etiological factors (causes) of diabetes mellitus in human subjects.
In 1958, he published the results of additional studies which confirmed his earlier work. His 1964 paper contained the very suggestive results of the work on the intestinal transport of glucose. It was found that the intestinal absorption of sugar was about doubled when the animals were deprived of ascorbic acid and returned to normal when they received ascorbic acid. If this observation is applicable to humans, it would mean that the intestines of diabetics,who may exist on chronic, low levels of ascorbic acid, would permit much more rapid absorption of sugar after eating. The blood sugar levels would rise to higher levels faster and put abnormal stress on the already strained insulin production in their pancreas.
Other workers have reached similar results. In fact, there have been so many papers published that a complete review is impossible in a single chapter. We will only discuss some very suggestive results on which further research should be expended. Altenburger, in 1936, showed that guinea pigs deprived of ascorbic acid were unable to convert glucose to glycogen for storage in their livers, but this condition was promptly relieved when ascorbic acid was administered. A dose of insulin that produced a pronounced decline in blood sugar in normal monkeys had little effect on monkeys deprived of ascorbic acid (Stewart and coworkers, 1952). The intimate relationship between insulin and ascorbic acid has been noted numerous times. When insulin is injected, there is a fall in the ascorbic acid levels in the blood serum of man, dogs, and rats, as shown by Ralli and Sherry in 1940 and 1948. Haid, in 1941, also noted this drop, not only after insulin injection but in patients in insulin shock. Previously, in 1939, Wille reported that ascorbic acid is helpful to schizophrenics receiving insulin shock treatments. She also produced evidence that ascorbic acid acts to raise the blood sugar levels in hypoglycemic attacks and said that prolonged administration of ascorbic acid will prevent these low blood sugar attache(3).
Ascorbic acid potentiates the action of insulin and, therefore makes it possible to derive the same effect with much less insulin. This was observed in 1939 by Bartelheimer and was accidently confirmed by Rogoff and coworkers in 1944. (4). Rogoff and his coworkers noted greater sensitivity in two diabetic children to their usual dose of insulin in the diabetic ward of their Pittsburgh hospital. On checking, they found that the children had also been given ascorbic acid and they believed this fact was responsible for the excessive insulin effect. In reviewing the literature, they cite a paper by Dienst, Diemer, and Scheer which reported that the ascorbic acid used in their tests on diabetics was equivalent to the effect of twenty units of insulin. They also mention the work of Pfleger and Scholl (40) who, in 1937, noted that ascorbic acid so improved the action of insulin that a diabetic could control his sugar tolerance with a lower level of insulin. Such conclusions should have initiated large-scale intensive research to determine how much ascorbic acid is needed to minimize the disagreeable insulin injections and still maintain controlled sugar metabolism and, incidentally, save diabetics millions of dollars. The combination of ascorbic acid with the oral medications may also be helpful in avoiding some of the undesirable vascular side effects of diabetic treatment(5).
Tests were started in the early 1930s to determine if the administration of ascorbic acid would reduce the blood sugar levels of diabetics and this resulted in a large volume of medical literature. As in the treatment of other diseases, with the short-term use of ascorbic acid, the more papers that appeared, the more confusion resulted. Some clinicians reported good results in controlling diabetes and others stated that there was no effect. The pros and cons are too numerous to be reviewed here. It was pointed out, in 1935,that the does used may have been insufficient (6). Whether or not this was true is unimportant; the entire approach to this research work may have been misdirected. The tests were aimed at the short-term application of ascorbic acid to see whether diabetes, caused by an already damaged pancreas, could be controlled. A better approach would have been in the area of prevention: the long-term administration of ascorbic acid to prevent pancreatic damage and the subsequent occurrence of diabetes. Such a plan is explained in the following paragraphs.
There is an assemblage of facts, scattered in the medical literature like pieced of a jigsaw puzzle, which have lain dormant for decades. But when put together, they form the picture for research to possibly prevent the millions of cases of diabetes which develop later in life, especially in individuals who carry the recessive gene for this trait. The pattern of the projected research would be to correct one genetic disease, hypoascorbemia, in order to help prevent the other, diabetes. Here are the facts
1. There is a substance called alloxan which, when injected into laboratory animals, produces diabetes. This has long been known and was used as far back as 1943 as a convenient and rapid means for inducing diabetes in laboratory animals for testing purposes.
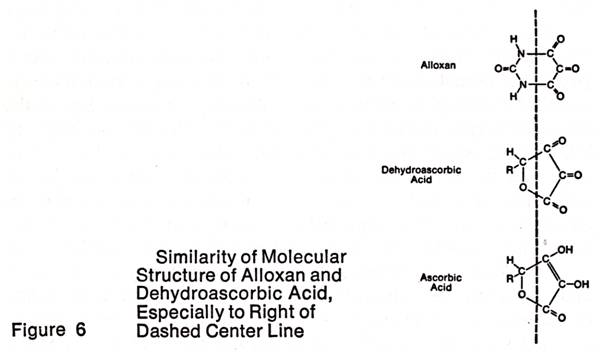
2. When ascorbic acid is oxidized, it forms dehydroascorbic acid, a compound similar in structure to alloxan. The structures of ascorbic acid, dehydroascorbic acid and alloxan are shown in Figure 6. One doesn't have to be a chemist to see the similarity between dehydroascorbic acid and alloxan structures to the right of the midline drawn through the molecule and the dissimilarity of ascorbic acid. The chemical properties of alloxan and dehydroascorbic acid are also strikingly similar, as noted by Patterson in 1950.
3. Like alloxan, the injection of dehydroascorbic acid into rats produces diabetes as was shown by Patterson in 1949 and also produces diabetic cataracts as he showed in 1951. That injection of ascorbic acid does not produce diabetes was shown by Levey and Suter in 1946.
4. Banerjee reported in 1952 that he found no dehydroascorbic acid in the tissues, including the pancreas, of normal guinea pigs but stated, "It was present in considerable amounts in the tissues of scorbutic guinea pigs: (7).
5. The mammalian genetic disease, hypoascorbemia, prevents us from making the mammalian liver metabolite, ascorbic acid. The full correction of this genetic disease provides the rationale for the intake of much higher levels of ascorbic acid (8).
The genetically potential diabetics are those who may develop the diabetic state later in life. During their early years, they have an apparent normal production and secretion of insulin from their pancreas. As a group, they are likely to be more sensitive to factors which may affect the delicate physiological balance which controls insulin production. This is indeed a delicate equilibrium. With too little insulin, diabetes is the result; too much insulin produces the equally serious disease, hypoglycemia. These genetically sensitive individuals have probably existed all of their lifetime on suboptimal levels of ascorbic acid. Even the best diet could not supply their individual requirements. Finally, chronic ascorbic acid deprivation and depletion pushes them over the brink into a state of abnormal insulin production. This chronic exposure of their pancreas to the consequent high ratios of dehydroascorbic acid may slowly damage the secretory cells beyond the point where normal function or regeneration is possible, and the abnormal sugar responses result.
Diabetes may be prevented by the long-term ingestion of daily optimal amounts of ascorbic acid to keep dyhydroascorbic acid-ascorbic acid ratios at a minimum. The long-term research needed to prove or disprove this thesis will be expensive, but preventing diabetes or hypoglycemia in millions of cases would certainly be worth all the costs.
24
____________________________________________________________
CHEMICAL STRESSES -- POISONS, TOXINS
One of the main functions of ascorbic acid in the mammalian body is to maintain normalcy under the effects of environmental stresses. To accomplish this, when under stress, most mammals merely produce more ascorbic acid in their liver. Stress covers a wide variety of conditions, and in this chapter we will discuss chemical stresses. The chemical stresses include such hazards to which we are exposed by contact, breathing, eating, and smoking; attacks by poisonous insects and reptiles; and the highly poisonous toxins of bacterial growth and infection. The amount of work expended over the past forty years on the use of ascorbic acid to counteract the bad effects of chemical stresses is voluminous and it is again impossible to completely cover the field. Even for a brief introduction to this subject, we must subdivide the topic. First, let us see what medical literature reveals about inorganic poisons.
Inorganic Poisons
The majority of the inorganic chemical hazards consist of the poisonous metals, such as the mercury in the seafood we eat, the lead in the paint chips killing ghetto children, the hazardous industrial metals, and the pharmaceutical metals like arsenic.
Mercury. In 1951, Vauthey showed that a certain dose of mercury cyanide injected into guinea pigs killed 100 percent of the animals within 1 hour. If, prior to this mercury injection, he kept his guinea pigs on megascorbic levels of ascorbic acid (equivalent to 35 grams a day for a human weighing 70 kilograms or 154 pounds), 40 percent survived the mercury poisoning. A similar protective effect against bichloride of mercury had been found ten years earlier by Mavin in Argentina. This was further confirmed, in 1964 by Mokranjac and Petrovic. Certain mercury compounds are used in medicine, such as diuretics (to reduce body fluids), which produce toxic reactions in patients. Chapman and Shaffer, in 1947, showed that the toxicity of certain mercurial diuretics could be reduced by prior or simultaneous administration of ascorbic acid. They also reported that in cardiac failure patients, a dose of only 150 milligrams of ascorbic acid increased the diuretic action by 50 percent. Further work on ascorbic acid and the mercurial diuretics was reported by Ruskin and Ruskin in 1952 (1).
Lead. In the 1939 report of a study of 400 workers in a large industrial plant, where exposure to lead hazards was great, Holmes and coworkers observed that the symptoms of chronic lead poisoning resembled subclinical scurvy. As an experiment, they used a group of seventeen people with chronic lead poisoning and gave them 100 milligrams of ascorbic acid daily. Within a week or less; "Most of the men enjoyed normal sleep, lost the irritability and nervousness so common with high calcium treatment of lead poisoning, enjoyed their food more and no longer had the tremors. Several cases of leukopenia [low white cell blood counts]... were cured by the ascorbic acid treatment."
Marachmont-Robinson, in 1941, working with 303 employees of an automobile body plant, where lead exposure was high due to the practice of soldering the seams with lad-containing solder and grinding it to a smooth finish, exposed workers to both lead fumes and lead dust. Beginning in June 1939, each worker was given two sticks of gum containing 50 milligrams of ascorbic acid at lunch. The author states, "This study confirms the contention of Holmes that vitamin C (ascorbic acid) has a detoxifying action on lead in the human body." He concludes with the statement "The routine administration of 50 milligrams of ascorbic acid daily appears to protect workers exposed to lead dust against the usual effects of chronic absorption" (2).
In tests on animals, Pillemer et al. (2) reported tests on guinea pigs poisoned with massive doses of lead carbonate (an old-time white paint pigment) and fed different levels of ascorbic acid. In discussion "paralysis, convulsions, and death," the report states:
Here the beneficial effects of a high ascorbic acid intake were striking and appear to be unequivocal. In both experiments only two of the twenty-six guinea pigs on the vitamin C regime developed clear-cut spasticities or paralysis, and none of the pigs died of lead poisoning during the period of observation. On the other hand, eighteen of the forty-four animals on the low ascorbic acid intake developed some form of neuroplumbism and twelve died of typical lead poisoning.
The so-called high and low intakes were respectively 50 milligrams and 2.5 milligrams per kilogram of body weight, assuming the guinea pigs weighed about 400 grams (the authors did not report the guinea pig weights). On this basis the daily ascorbic acid intakes for an adult human for their "high" successful series would be 3,500 milligrams and for their "low" ineffectual series, 155 milligrams. But even this ineffectual level is more than twice the current daily recommended allowance for man.
At this point, we will discuss the short note appearing in 1940 in which Dannenberg et al. (2) conclude, "Extremely large doses of ascorbic acid were without effect in the treatment of lead intoxication in a child aged twenty-seven months." From the time the child was fifteen months old, it had eaten wood, paper, and painted articles. When first seen it was a very sick, thirty-six pound, twenty-seven-month-old boy and a diagnosis was made of chronic lead poisoning and lead encephalosis. For seventeen days the little boy was given 100 milligrams daily of ascorbic acid in divided doses and a daily injection of 250 milligrams ascorbic acid, for a total of 350 milligrams per day. For perspective, this calculates only to about 1.5 grams a day based on a 150-pound adult. A blood examination showed the lead content to be over twelve times higher than normal. After seventeen days, the child showed no improvement and was taken off the "high" ascorbic acid and other therapy was substituted which still included 50 milligrams of ascorbic acid a day. The child was discharged eighty-three days after admission, but still not completely free of the after-effects of the lead intoxication. It is likely in this case that the lead poisoning was so severe that the so-called extremely large doses of ascorbic acid were insufficient to cope with the problem. The fact that the child did not die in the first few weeks after hospitalization and slowly recuperate is probably an unrecognized tribute to the value of ascorbic acid.
In 1963, Gontzea and coworkers (2) studied the blood ascorbic acid levels in long-term workers in a lead-storage battery plant. The blood levels were found to be low and they concluded that persons exposed to lead require larger intakes of ascorbic acid to avoid subclinical scurvy.
In further tests on animals, three Chinese workers, W. Han Wen et al., kept a hundred tadpoles in water with high lead content for twenty-four hours and eight died. The living tadpoles were divided into tanks containing plain water as a control and plain water containing 31 mg% of ascorbic acid. Six days later, all the tadpoles in the ascorbic acid treated water were alive, while 88 percent in the plain water had died. Uzbekov, in 1960, reported the results of his tests on lead-poisoned rabbits using ascorbic acid and cysteine. He concluded that this combination should not only be used in the treatment of lead poisoning but also as an antidote (2).
Arsenic. In the early 1940s, various arsenical compounds were in current use for the treatment of syphilis. These compounds produced toxic reactions in the patients and many papers were published showing the detoxifying properties of ascorbic acid when used in combination with these arsenical drugs. Typical are the reports of McChesney and associates, and Abt, in 1942; Lahiri, in 1943; and McChesney, in 1945. Lahiri states, "The administration of vitamin C is the safest way of avoiding arsenical intolerance in antisyphilitic therapy." In 1962, Marocco and E. Rigotti showed that ascorbic acid prevented kidney damage in arsenic poisoning (3).
Chromium and Gold. The recent work of Samitz and coworkers (4) has shown that ascorbic acid can be used to prevent chromium poisoning and chrome ulcers in industry. Gold salts are used medicinally and have toxic actions on the patient which can be prevented with ascorbic acid, as shown in Brazil in 1937 and 1940 (5).
In the above review we have covered the poisonous metals (Mercury, lead, chromium, and gold) and a nonmetal (arsenic). In each case ascorbic acid was shown to counteract the poisonous effects. Yet all this suggestive work has apparently been ignored, particularly in two current serious problems: first, the deaths or long-term damage of children from eating paint chips containing lead, and second, exposure to high mercury levels in certain seafoods.
ORGANIC POISONS
Benzene Poisoning. Benzene is a component in various chemical manufacturing processes, such as DDT production, and workers may be exposed to vapors from this volatile ingredient. Many papers, dating back to 1937, have been published showing that exposure to benzene depletes the body of ascorbic acid, that this brings on a state of subclinical scurvy, and that the administration of ascorbic acid helps prevent and alleviate the symptoms of chronic benzene exposure. The 1965 paper by Lurie gives an excellent review and many references to the early literature. Lurie was able to eliminate chronic benzene poisoning among the workers in a South African chemical plant by seeing to it that they received some ascorbic acid in a daily ration of orange juice. In the Czech paper by Thiele, in 1964, he states the chronic benzene poisoning causes, "...vitamin C deficiency without signs of scurvy, [and] toxic damage of the capillaries and excessive bleeding." These latter symptoms are characteristic of prolonged deprivation of ascorbic acid. Forssman and Frykholm, in 1947, reported from Stockholm that, "exposure to benzene creates an increased need of vitamin C and that an extra supply of vitamin C gives increased resistance to the effects of benzene." A Russian paper by Bilpov appeared which showed that rats reacted to DDT injections by producing more ascorbic acid. This would indicate that ascorbic acid might be useful in the treatment of DDT poisoning in man and other animals; however, no further work in this critical area was noted (6).
Drugs. The effectiveness of drugs in therapy is limited by their toxic actions on the body. The dosages employed are a compromise between their therapeutic effect and their poisonous effect. Ascorbic acid has long been known to detoxify the poisonous effects of various drugs and to potentiate their therapeutic effects.
The highly poisonous convulsive drug, strychnine, is rendered harmless with ascorbic acid as shown by Dey (7) in 1965 and 1967. All of his mice died when injected with 2 milligrams per kilogram of body weight of strychnine, whereas if the mice were first injected with ascorbic acid 15 minutes before administration of strychnine, they did not die. With ascorbic acid at 100 milligrams per kilogram of body weight, there was 60 percent survival; with 1,000 milligrams per kilogram of body weight, none of the poisoned animals died. For a 70-kilogram animal, the size of a human adult, this would be equivalent to 7 grams and 70 grams of ascorbic acid respectively. Day also pointed out that his observations might be useful in the treatment of tetanus (lockjaw), which we will discuss later.
In 1959, Schulteiss and Tarai (7) suggested the use of ascorbic acid to avoid the harmful side effects of digitalis therapy of heart disease in the aged. Ascorbic acid reduces the toxicity and side reactions of the sulfa drugs. The toxic effects of aspirin are alleviated by ascorbic acid. Too much vitamin A induces a scurvylike syndrome which is promptly relieved with ascorbic acid as shown by Vedder and Rosenberg in 1938 (8).
In acute poisoning by barbiturates, a 1965 Chinese paper (9) showed that intravenous administration of large doses of ascorbic acid had a therapeutic effect on relieving the depression of the central nervous system caused by the drug. It increased the blood pressure and respiration, and produced more forceful heartbeats. Ten years earlier Klenner reported on this successful treatment of barbiturate poisoning by injecting 54 grams of ascorbic acid on the first day.
A 1960 paper by Ghione (9), from Ghione (9), from the University of Rome, reported that ascorbic acid at 100 milligrams per kilogram of body weight attenuated and abolished the effects of morphine in rats. With the narcotics problem among our young people reaching such vast proportions it is a sorry commentary that these observations and others on the efficacy of ascorbic acid have not been the basis of a crash research program to help solve some of the addiction problems. Most addicts and smokers of Marijuana are probably in a severe state of subclinical scurvy. It may be possible to utilize megascorbic levels to aid in the treatment of addiction and to relieve the drug withdrawal symptoms. By relieving the subclinical scurvy and maintaining their health at a higher level, it may serve to prevent backsliding to the drugs. We will never know unless the appropriate research is conducted.
A paper on anesthesia and ascorbic acid, in the literature since 1944, should have elicited wide responses in surgery. Beyer and coworkers (10) found that the use of anesthetics had a profound influence on the blood levels of ascorbic acid in dogs. They also found that nonscorbutic, ascorbic acid-deprived guinea pigs became anesthetized sooner and deeper. Recovery was slower and the guinea pigs showed more prolonged toxic aftereffects than animals with adequate ascorbic acid. In one test using chloroform, the acid-deficient animals died from respiratory arrest under conditions which only induced light anesthesia in the ascorbic acid-protected group. I wonder whether in the last twenty-five years any further tests were made to explore these observations and if any hospitals bother to check the ascorbic acid adequacy of their patients before subjecting them to anesthesia? Further exploration may improve the chances for patients undergoing surgery.
Bacterial Toxins. The toxins are a group of poisons of protein-like nature which may be produced by certain pathogenic bacteria, by insects such as spiders and scorpions, and by poisonous snakes. We will discuss the bacterial toxins first.
The toxins of certain disease-producing bacteria are among the most poisonous substances known. They symptoms and morbidity of the disease are due not so much to the presence of these bacteria, but to the toxins they produce. Much work was expended in the 1930s on the diphtheria toxin and its inactivation by ascorbic acid, but since diphtheria is no longer much of a problem, we will start our discussion with the more important tetanus toxin and its consequent disease, lockjaw.
Tetanus. Every time you suffer a deep cut, you are a potential victim of the serious, life-threatening disease, tetanus. The spores of the germ Clostridium tetani have a wide distribution and are especially abundant in the soil. The germs are anaerobes and cannot grow in the presence of air. Because of this, they only infect deep cuts out of contact with air. The usual treatment is to give a prophylactic injection of tetanus toxoid or antitoxin.
According to Bytchenko of the World Health Organization, tetanus has killed more than a million people in the last ten years, "killing more than smallpox, rabies, plague, anthrax, and polio, yet it receives less attention by public health authorities and medical science than any of these."
If the disease develops in spite of precautions, the patient is in trouble. Current treatment is nearly as bad as the disease itself. There is definite need for an improved therapy and ascorbic acid may be the basis for it if only the research would be conducted.
The 1966 paper by Dey (11) reports on tests with groups of animals given the same amount of tetanus toxin. In the first group given the toxin alone, all animals perished in 47 to 65 hours. The second group, in which ascorbic acid was given (1 gram per kilogram of body weight) at the same time, and then twice daily for three days, all animals survived and only very mild symptoms appeared. Animals of the third group received the ascorbic acid for three days prior to the toxin inoculation and then for three days after. All these animals not only survived, but did not show any symptoms of the poisoning. A fourth group was comprised of animals given the toxin, and the ascorbic acid was withheld until the tetanic symptoms appeared, usually sixteen to twenty-six hours later. They were then inoculated with ascorbic acid (1 gram per kilogram of body weight) twice daily for three days. The ascorbic acid prevented the spread of the symptoms and they all survived. In the fifth group, the ascorbic acid administration was further delayed for forty to forty-seven hours until there were marked symptoms of the disease and all the animals survived. Here is the nucleus of successful results which should have initiated wide-scale research into a disease for which modern medicine has failed to produce an effective treatment. The dosages used by Dey, if scaled up to the size of a human adult of 70-kilogram weight, are equivalent to 140 grams a day. Some will regard this amount as a heroic measure, but it is not far from the 70 grams a day used intravenously for reducing the intraocular pressure in human glaucoma. Further research would indicate the proper dose to be used.
It is of further interest and importance that Klenner, in 1954, reported on the successful treatment of tetanus with massive doses of ascorbic acid. Even long before, in 1938, we find that Nitzesco and coworkers reported inactivating tetanus toxin with ascorbic acid. The details of the needed research will be discussed after we look into the related problem of botulism (11).
Botulism. Botulism is a deadly type of food poisoning caused by the ingestion of the toxins produced in foods by the growth of the bacteria, clostridium botulinum. This is a germ closely related to the one causing tetanus and grows in nonacid foods in the absence of air. Improperly preserved packaged foods are the main source of this toxin. The onset of the symptoms is abrupt and the mortality may be as high as 65 percent. Five different types of botulinus toxins have been identified, each one requiring its own antiserum for treatment of the disease. The results of treatment with the antiserum are disappointing once the symptoms appear, but the treatment may be effective if applied before the onset of symptoms. Clearly, present therapy is rather primitive and a more effective treatment is needed. The detoxicating powers of ascorbic acid are will known and its action on increasing the survival of animals treated with many related bacterial toxins was reported in 1930 by Buller-Souto and Lima (12). In view of this, it is indeed surprising that use of ascorbic acid as a possible means of therapy and survival in botulism has not been further explored over the past three decades.
Research should be immediately initiated because the problem is pressing and more lives will be lost the longer it is delayed.
The research on tetanus, botulism, and other important bacterial toxins could be combined in initial experiments on guinea pigs and monkeys. Inoculating them with lethal amounts of the toxins and determining the correct amount of ascorbic acid (as sodium ascorbate and administered intravenously) required to permit survival and eliminate the symptoms of these intoxications could be the first step. The amounts used will be in the megascorbic range as established by Dey and Klenner (11).
Snakebite. There are about 2,500 species of snakes throughout the world and about 10 percent are venomous. This minority causes about 30,000 to 40,000 deaths each year, mostly in Asia. In the United States, about 7,000 people are bitten annually, of which about 40 to 60 percent are children and young adults. The regions of highest incidence are the southern and western states and in the period from 1950 to 1959 there were 158 snakebite deaths in this country. The usual treatment consists of supportive measures and injection of antivenin. It is necessary to identify the snake involved in order to obtain the correct type of antivenin since they are highly specific. For instance, the antivenin for the pit vipers is not recommended for the coral snakes. Since time is of the essence in treating a snakebite, a general treatment based on a more widely available material than antivenin and one limited by the high specificity for certain snakes would be highly desirable.
There have appeared suggestive reports on the use of ascorbic acid for treating snakebites which have never been properly explored. In 1938, Nitzesco et al. (11) showed that ascorbic acid when mixed with cobra venom rendered it harmless. Guinea pigs injected with the venom-ascorbic acid mixture, not only all survived, but did not even show any of the snakebite symptoms. They also emphasized the importance of high dosages. With 25 milligrams of ascorbic acid, all the animals survived; with 10 milligrams, the guinea pigs survived for a while, but eventually died; and with 5 milligrams there was no beneficial effect.
A 1947 paper from a Bogota', Columbia, oil company hospital (13) describes the dramatic emergency treatment of three snakebite cases where the biting snakes were not identified. The victims were first given the local treatment of incision of the wound, suction and tourniquet plus the oral administration of orange or lemon juice. They injected 2 grams of ascorbic acid intravenously every 3 hours. The author, Dr. Perdomo, states that immediately after the first injection of ascorbic acid a very favorable response was noted and, after subsequent injections, there was a complete elimination of all symptoms. The patients were observed up to a week later and showed no general or local complications. A plea was made for more research.
In a 1943 paper from India, kahn (13) reported that ascorbic acid was ineffective for preventing death in dogs injected with cobra venom. On examination of his experimental conditions, we find that he used only one injection of ascorbic acid to counteract the lethal dose of cobra venom. This dose amounted to only 70 to 140 milligrams of ascorbic acid per kilogram of body weight. Dey (11) required 1,000 to 2,000 milligrams of ascorbic acid per kilogram of body weight to counteract the lethal effects of tetanus toxin. In his dogs Kahn used less than 1/3 to 2/3 of the ascorbic acid dosage employed by Perdomo in humans and between 1/7 and 1/3 of the dosage suggested by Dey. If is likely that, if Kahn's tests were repeated using higher levels of ascorbic acid, the results would be as successful as the others.
Klenner, in 1953, alsi indicated the usefulness of ascorbic acid for snakebites. In a recent personal communication, he stated that he has not only successfully treated cases of snakebite in man megascorbically, but also in dogs, which totally contradicts Kahn's remarks. In 1957, he also revealed the usefulness of ascorbic acid in treating black widow spider bites. Similarly McCormick, in 1952, used ascorbic acid in the treatment of scorpion stings (13).
Here we have the basis for a simple and apparently harmless and effective treatment for a wide variety of animal toxins which has been ignored, for many years. Further exploration of these known facts, using a procedures similar to the tests suggested previously for tetanus and botulism, may provide a new, effective, and immediate treatment for snakebites, black widow spider bites, scorpion stings, and serious multiple bee stings by the mere intravenous infusion of sodium ascorbate at megascorbic levels. The groundwork has been laid for further exploratory research.
The above discussions are devoted to the bacterial and animal toxins, but ascorbic acid would probably be as effective against the plant toxin, such as mushroom poisons, as is indicated in the 1938 paper by Holland and Chlosta (14). Still their plea for further research remains unanswered to this very day.
The body has other biochemical pathways of detoxication besides ascorbic acid and the liver is usually referred to as the organ of detoxication. Nature moved the ascorbic acid-synthesizing enzymes into the liver during the evolution of the mammals. The liver thus became a much more efficient organ of detoxication, protected against the tissue-damaging effects of the various poisons which were concentrated in the liver. The protective action of ascorbic acid against liver damage was shown in 1943 by Beyer and again in 1965 by Soliman et al. (15). Additional research might show that long-term prophylactic megascorbic intakes may prevent cirrhosis and fatty degeneration of the liver which occur in those chronically exposed to toxic levels of various materials. One group that might benefit from further work in this area is the large number of alcoholics who eventually suffer from liver damage and cirrhosis.
25
____________________________________________________________
The physical stresses include exposure to heat and cold, physical trauma, burns, noise, high altitude, drowning, and ionizing radiation.
The usual mammalian response to stress is increased secretion of the hormones of the adrenal gland. This increased adrenal activity depletes ascorbic acid from the gland, which normally contains a higher concentration of ascorbic acid than any other body tissue. In mammals which produce their own ascorbic acid, this depletion is rapidly replenished. In the guinea pig, some monkeys, and man, the depletion is made up by robbing the body of its tissue stores of ascorbic acid. If the tissue stores are low, adrenal ascorbic acid may be insufficiently restored and the normal adrenal hormonal response to continued stress may become inadequate.
In 1952, Pirani (1) published a review of the work of the first twenty years of the ascorbic acid era. In the bibliography there were 242 references on the relationship of ascorbic acid to stress phenomena. Here again, we are confronted with a mass of literature from which we can select only a few. The conclusion reached in this review was that under normal conditions, the tissue stores are adequate to cope with acute stress. However, during severe chronic stress, especially after traumatic injuries or burns, and during protracted stimulation of the adrenal cortex, administration of ascorbic acid is indicated.
Heat and Burns
In a paper on "artificial fever" in which guinea pigs and human subjects were exposed to high environmental temperatures, Zook and Sharpless, in 1938, showed that high temperature exposure accelerates the destruction of ascorbic acid and increases the physiological need for it. Twenty-one years later, Thompson and coworkers confirmed this on women living in southern Arizona. They demonstrated that the rate of depletion of ascorbic acid in blood serum was significantly higher in summer than in winter. The basal metabolism, in a majority of their subjects, also diminished significantly in the summer. They stated, "It is apparent that ascorbic acid metabolism was altered in some manner due to increased requirement or destruction" (2).
In 1944, a paper by Henschel and coworkers (2) was published on short-term tests on the ability to work in hot environments. The subjects had been exposed to high temperatures from three hours to four days, under rigidly controlled environmental, dietary, and work conditions. Some of the subjects had been given 500 milligrams of ascorbic acid a day. This work was summarized as having "failed to demonstrate any significant advantage for men receiving supplements of ascorbic acid."
Then along in 1948 came the report by Weaver (2) on the prevention of heat prostration describing long-term tests on workers in a Virginia rayon plant who had been exposed to high temperatures and humidities. Weaver found that he was able to eliminate heat prostration in the employees by the daily administration of only 100 milligrams of ascorbic acid. Before instituting this regimen in 1938, there had been twenty-seven cases of heat prostration; in the following 9 years not a single case was reported in the group taking the daily 100 milligrams. During the discussion following the presentation of this paper, Dr. Weaver described the case of heat prostration in a subcontractor who was brought to his medical department at 3 P.M. in collapse and cyanotic. He administered 500 milligrams of ascorbic acid intravenously and by 6 P.M. the man was able to walk to his car and return home. He was back on his job the next day.
A similar test, conducted in the high temperatures near the furnaces of a steel plant, on combinations of salt tablets with vitamins, failed to show any benefits from the vitamins. In this study, Shoudy and collings administered even less ascorbic acid than the marginal levels used by Weaver. In any further clinical work conducted int his area, megascorbic levels of sodium ascorbate should be used, Sufficient sodium ascorbate must be available to maintain homeostasis under the sever heat stresses. Weaver used only about 1 milligram per kilogram of body weight. Agarkov reported in 1962 that 15 milligrams per kilogram of body weight improved the heat resistance of rate (2). Further studies are required to assess the proper usage of ascorbic acid in heat stress.
The use of ascorbic acid in the treatment of severe burns has been neglected, even after Klasson (3) published his dramatic results in 1951. His basic procedures might have eliminated suffering and saved the lives of many fire victims over the past twenty years if it had been more widely used. Klasson reported don sixty-two burn cases from a variety of causes such as hot water, hot grease, gasoline explosions, and chemical agents. He used ascorbic acid topically, by mount, and intravenously. He applied a 1 percent ascorbic acid solution in 0.9 percent salt solution or a 2 percent ascorbic acid ointment in a water soluble base directly to the burned area. When these were applied, there was immediate relief from pain, which permitted a reduction in the morphine given the victims. Spraying the throat or gargling with a 1 percent ascorbic acid in normal saline solution, rapidly alleviated the hoarseness and pain caused by swallowing smoke. In addition, Klasson gave up to 2,000 milligrams of ascorbic acid a day by mouth or intravenously and at "no time were deleterious effects from the drug observed." In severe burn cases, there is usually a suppression of urine and Klasson found the ascorbic acid treatment maintained the urinary output at normal levels. He summarized his study by stating that ascorbic acid alleviates pain, hastens healing combats the accumulation of toxic protein metabolites in severe burn cases, and reduces the time needed before skin grafting.
Klenner (4), in 1971, stated he had found the "secret" for reducing paid and infection form severe burns, preventing toxemia and promoting healing. This method is summarized in the following five steps: 1. The patient is kept unclothed without dressings in a warmed cradle. 2. A 3 percent solution of ascorbic acid is sprayed over the entire burned area every two to four hours for about five days. 3. Vitamin A and D ointment is then alternated with the 3 percent ascorbic acid spray. 4. Megascorbic doses are administered by mouth and by vein of 500 milligrams of ascorbic acid per kilogram body weight as sodium ascorbate (35 gram for a 70-kilogram adult) every eight hours (105 grams a day) for the first several days, then at twelve-hour intervals (1 gram calcium gluconate is given daily to replace calcium lost in body fluids). 5. Supportive treatment is given.
What more suggestive and promising leads are required to start a program of research to explore a new treatment for burns to replace the rather primitive methods now used? Klasson cites fifteen references from the medical literature, dating back to 1936, which lead him to try ascorbic acid. Later work (5) showed the profound influence of burns on the ascorbic acid metabolism, but no group bothered to conduct the large-scale crucial clinical trials using ascorbic acid or sodium ascorbate at megascorbic levels (topically, orally, and intravenously), to develop an improved therapy.
Cold
There is a considerable medical literature on cold temperatures and their effect on the ascorbic acid in the body. Outstanding are the investigations of the Canadian Dugal and coworkers, starting in 1947, continuing for many years, and summarized in 1961. In their 1947 paper (6), they reported rats, which were exposed for long periods to freezing temperatures,but which were able to adjust to these low temperatures, had large increases in the ascorbic acid levels of their body tissues; whereas, those rats unable to adjust to the cold environment had decreased levels. They concluded that maintenance of life at low temperatures requires large quantities of ascorbic acid. This was further confirmed with tests on guinea pigs.
In long-term tests on monkeys reported in 1952, Dugal and Fortier (6) found that among monkeys exposed for six months to cold temperatures (50oF) and then subjected to subfreezing temperature (-4oF) those given 325 milligrams of ascorbic acid daily for the six month period were far more resistant to the intense cold than those given only 25 milligrams a day. Since their monkeys weighed about 12.5 pounds, this calculates to 4,000 milligrams or 4 grams, a day based on the weight of a human adult (70 kilograms) for the cold-resistant group and about 300 milligrams daily for the group showing no resistance.
No tests have been conducted to determine if the resistance of humans to cold temperatures could be improved using 4 grams or more of ascorbic acid. One short-term test (thirteen days) on soldiers, reported in 1954,employed only 525 milligrams of ascorbic acid a day in one group and 25 milligrams in another. Both groups were exposed to cold temperatures on survival rations. The group on the high, but sill marginal levels of 525 milligrams, showed improved resistance to the cold and a large decrease in foot troubles over the 25-milligram group. In another short-term test reported, in 1946, Glickman and coworkers broadly concluded that the results of their experiment indicated clearly that the ability of men to withstand the damaging effects of repeated exposures to cold environments cannot be appreciably enhanced by giving "excessive" doses of ascorbic acid or other vitamins above the amounts required for adequate nutrition. However, their idea of an "excessive" dose of ascorbic acid was 200 milligrams a day, which had been shown to be ineffective in the monkey experiments previously mentioned (6). We cannot say, at this point, whether the megascorbic levels will improve human resistance to cold or not, but if further tests are to be conducted, they should use at least the levels found successful in monkeys. There are millions of people suffering each year from the effects of winter cold who may benefit if these tests yield successful results.
Physical Trauma
Ungar (7), a member of the Free French Forces studying wound ballistics, provided information of vital importance which might have saved the lives of thousands of soldiers and auto accident victims if it had been properly followed up. The purpose of his study was to relate the degree of trauma expressed in terms of physical energy with the severity of shock as estimated by mortality. Ungar took anesthetized guinea pigs and dropped known weights from different heights onto the animals and found there was a definite relationship between transmitted energy and tissue damage and mortality. The startling fact brought out by his research was that in guinea pigs subjected to the dropped weights, which ordinarily would kill 100 percent of the animals, these animals would always survive if given an injection of ascorbic acid in doses about 100 milligrams per kilogram of body weight shortly after the trauma. His injection dosage calculates to over 7 grams of ascorbic acid, based on a 70-kilogram body weight. The prompt administration of this amount or more of ascorbic acid in the battlefield to wounded soldiers or to auto accident victims at the scene may prevent shock and ensure survival until they reach a hospital. You might well ask how it is possible for such an important observation to lay dormant for 30 years.
Bone Fracture
The 1946 paper by Andreae and Browne (7) showed that tin man, both burn and bone fracture trauma produce rapid decreases of ascorbic acid in the whole blood and the white blood cells.
A 1962 paper from the Soviet Union by Merezhinskii (7) reported tests on guinea pigs with bone fractures. Merezhinskii showed the the daily administration of 40 milligrams of ascorbic acid was sufficient to correct for the ascorbic acid losses due to the trauma but 10 milligrams were not. He found that the recovery from bone fractures was considerably shortened when large doses of ascorbic acid were given. His successful 40-milligram dose, when scaled up to a 150-pound body weight, amounts to the daily intake of about 9 grams of ascorbic acid, while his inadequate 10-milligram dose is equivalent to 2.3 grams a day.
High Altitude
Exposure to high altitude is a severe form of stress because the rarefied atmosphere induces oxygen deprivation, known as hypoxia. Hypoxia is a lack of the proper levels of oxygen in the blood and tissues. Severe hypoxia can be induced in the body by means other than high altitude, such as drowning. Our discussion of high altitudes will also apply to these other conditions.
If people are transported from sea level to high mountainous altitudes, there is a chance that they will develop acute mountain sickness before they become accustomed to the great heights. The disease is called soroche in the Andes and probably has many other local names in various mountain areas. The air we breathe contains about 20 percent oxygen at sea level but only about 15 percent at about 15,000 feet. High altitude was also a problem in aviation before the advent of the pressurized cabin,
As long ago as 1938 it was perceived that ascorbic acid increases the altitude tolerance of ski troop and rabbits. Peterson, in 1941, showed that mice injected with ascorbic acid were able to withstand repeated exposure to air pressures that were 1/6 normal, while their untreated companions succumbed. Krasno and coworkers showed in 1950, using human subjects repeatedly exposed to 18,000-foot altitude conditions, increased utilization of ascorbic acid with consequent depletion. This was confirmed in guinea pigs exposed to the same high altitudes, with the animals manifesting abnormally low levels of tissue ascorbic acid. In a 1959 paper from Yugoslavia, Wesley and coworkers reported that in guinea pigs exposed for one hour to low air pressures equivalent to a 30,000-foot height, there was a drop in ascorbic acid levels and a substantial increase in the more toxic dehydroascorbic acid levels. This was also confirmed in dogs; and tests were made on men who responded similarly to the hypoxia, depending upon the intensity and duration of exposure (8).
Even with this extensive background of suggestive research, I was unable to find anyone who was inspired to prevent altitude sickness or the bad effects of hypoxia by the administration of high levels of ascorbic acid. The closest to a test of this nature was reported by Brooks (8), in 1948, using the dyestuff, methylene blue. She found that if people who normally suffered from altitude sickness were given 0.2 grams of the methylene blue before ascending to about 15,000 feet in a four-hour automobile trip, they no longer became ill. Also, untreated subjects who became ill with headache and nausea at 10,000 feet, if given 0,1 gram of methylene blue, were free of the symptoms within an hour. Methylene blue and ascorbic acid a re both members of oxidation-reduction systems and should have similar therapeutic actions. Anything methylene blue can do, ascorbic acid should do better. The diuretic effect of ascorbic acid should also help relieve the pulmonary edema that develops at high altitudes. It is time now for the necessary further clinical work, since hypoxia is a widespread problem much beyond altitude sickness. The results obtained would be important in the treatment of the hypoxia of nonfatal drownings, of infants during birth, during anesthesia in surgery, in prolonged surgical procedures, and in suffocation cases, to prevent brain damage.
Radiation
Exposure to radiation is an extremely stressful situation for the living organism. The term "radiation" includes ultraviolet rays, X rays, gamma rays, and other ionizing radiation in the radiant-energy spectrum. The dangers of exposure to X rays have been recognized in recent years and the radiation casualties of the atom bombings are proof of the hazards. Exposure to radiation, as an occupational hazard for physicians specializing in radiology, has had a life-shortening effect and has increased susceptibility to disease, as compared to physicians in other specialties (9).
There have been numerous papers published showing that exposure to X-rays lowers the levels of ascorbic acid in the body: Kretzschmer et al., in 1947; Monier and Weiss, in 1952; Hochman et al. and Oster et al., in 1953; Dolgova, in 1962; and many other papers from the Soviet Union from 1963 on (10). In general, these papers indicate that in guinea pigs, which cannot synthesize their own ascorbic acid under stress, there are decreases on ascorbic acid in the blood and tissues after irradiation. Animals, such as rats and rabbits, that produce ascorbic acid in their livers under stress usually suffer an initial drop in their ascorbic acid level which rises after the liver has had a chance to replace the lost ascorbic acid. If the irradiation is severe enough to interfere with the synthesis of ascorbic acid, the losses remain.
The use of ascorbic acid as a protection against the unfavorable effects of radiation goes back many years and, in spite of the fact that the investigators used pitifully small doses of ascorbic acid, many reported good results. Carrie and Schnettler, in 1939, using only 200 milligrams a day of ascorbic acid, reported good results and recommended it as the medication of choice. They were able to prevent the leukopenia (reduction of white blood cells in the blood) induced by exposure to X rays. This was confirmed by Clausen, in 1942, who prevented the leukopenia in ten stomach- cancer patients treated with X rays by giving them a daily injection of 500 milligrams of ascorbic acid. Wallace, in 1941, injected only 50 milligrams of ascorbic acid daily and was able to report that it prevented many general symptoms of radiation sickness and almost entirely eliminated the severe nausea and vomiting, but it did not prevent the intestinal changes due to the heavy pelvic X-ray treatments administered (11).
Kalnins, from Sweden, who published many other papers in this area, reported in 1953 that the X-ray lesions of guinea pigs given 50 milligrams a day of ascorbic acid were much better protected against the damaging radiation effects than those given only 1 milligram a day. He thought that the large doses of ascorbic acid acted as detoxicant for the histamine‑like bodies or the leukotoxins developed in the irradiated tissue. Yusipiv, from the Soviet Union, in two short papers reporting tests in 1959 on rabbits and rats that did not specify the dosages of ascorbic acid he used, indicated that if ascorbic acid was given before the irradiation, it exerted an unfavorable effect, but if administered afterward it was beneficial. He recommended the use of ascorbic acid in the treatment of acute radiation sickness in the latent period and period of climax. He mentions that the clarification of the role of ascorbic acid in acute radiation sickness is one for the immediate future (11). Several papers have appeared showing the protective effect of ascorbic acid on various bodily enzymes against destruction by ionizing radiation. In the 1965 paper by Shapiro et al. (12), the scientists suggested the comprehensive testing of ascorbic acid as a radiation-protective agent in animals.
Although the usefulness of ascorbic acid has been indicated, the crucial clinical tests, using the higher levels of ascorbic acid, have not been initiated. These long-overdue tests should be started and thoroughly explored.